- By - Malfaifi
- Posted on
- Posted in Diagnosis, Fixed, Prosthesis
Worn dentition
Restoration of the extremely worn dentition
Turner and Missirlian 1984

This article discusses the diagnostic evaluation, treatment planning, and modes of restorative treatment for patients who suffer from extreme occlusal wear.
Etiology of tooth wear:
- Congenital anomalies:
- Amelogenesis Imperfecta: (hypoplastic, hypomaturation, hypocalcified).
- Dentinogenesis imperfect: is characterized by an amber-colored translucency of the denti- tion, and because of a weakened attachment between the normal enamel and the affected dentin, the enamel has a tendency to shear and expose the relatively soft dentin subject to rapid and extensive attrition.
- Parafunctional occlusal habits
The effect of chronic bruxism and other oral habits such as biting on needles, pipe stems, pencils, and hairpins, if continued over an extended period of time, is often attrition of tooth structure.
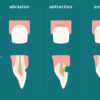
- Abrasion: tooth wear by external agent.
- Erosion: tooth erosion may result from excessive intake of citrus juices, and other beverages that contain carbonic acid, vinegar, and pickled foods.? Medicaments, such as hydrochloric acid prescribed for achlorhydria, may also eventually cause tooth erosion. Patients who continuously regurgitate stomach contents into the mouth commonly exhibit perimyelolysis on the lingual surfaces of the maxillary anterior teeth. Chronic vomiting may be self-induced in patients who suffer from psychosomatic. disorders such as anorexia nervosa.
- Loss of posterior support: Extensive attrition of anterior teeth often occurs when posterior support has been compromised by loss of teeth, malposition of teeth, or occlusal interference that drives the mandible forward and exerts undue force on the anterior teeth.
Evaluation of occlusal vertical dimension It is commonly assumed that extensive occlusal wear results in decreased occlusal vertical dimension. There is no definitive evidence to support this concept. However, the literature is replete with reports that rehabilitation of an increased occlusal vertical dimension may cause postoperative problems and should be avoided when possible. Therefore, it is critical to verify loss of occlusal vertical dimension prior to restoration at an increased occlusal vertical dimension.
Methods of evaluation
- Loss of posterior support: it is the most common factor that cause ant. teeth wear and loss of VDO
- History of wear: Gradual occlusal wear over many years is generally compensated by continuous eruption. Accelerated breakdown and wear exceeds the rate of eruption and results in decreased occlusal vertical dimension.
- Phonetic evaluation: The normal mandibular position during the/S/sound places the incisal edge of the mandibular incisors about 1 mm inferior and lingual to the incisal edge of the maxillary incisors. Vertical positioning significantly more than 1 mm apart may indicate lost occlusal vertical dimension.
- Interocclusal distance: Methods of measuring interocclusal distance are diverse, inaccurate, and inconsistant. Therefore, the measurements should be used only as a supplemental diagnostic aid for evaluating occlusal vertical dimension of the worn dentition.
- Facial appearance: The external appearance of facial tissues and musculature should be carefully reviewed if loss of vertical dimension is suspected. Diminished facial contour, thin lips with narrow vermillion borders, and drooping commissures are associated with overclosure
Alternative treatment plans
– Category No. 1. Excessive wear with loss of occlusal vertical dimension : Typically for patient with loss of posterior support the only reliable method to confirm the diagnosis and determine a physiologic occlusal vertical dimension is with trial restorations (Occlusal splints).
The patient should be re-checked periodically for 6-8 weeks to evaluate patient comfort.
Category No. 2. Excessive wear without loss of occlusal vertical dimension but with space available : long history with gradual tooth wear and worn teeth over erupt to compensate the loss of vertical In these patients continuous eruption has maintained occlusal vertical dimension, but there is seemingly insufficient interocclusal space for restorative materials unless occlusal vertical dimension is increased.
Category No. 3. Excessive wear without loss of occlusal vertical dimension but with limited space : Restoration of the worn dentition of a patient in category No. 3 is the most difficult because vertical space must be obtained for restorative materials.
This can be accomplished by orthodontic movement, restorative repositioning, surgical repositioning of segments, and programmed occlusal vertical dimension modification.
Conclusion:
Careful evaluation of the etiology, history, and factors relative to occlusal vertical dimension are essential to appropriate treatment planning. Various modalities are successful in the treatment of patients with a worn dentition.