Maxillary Sinus Floor Elevation: A Valuable Pre-prosthetic Procedure
Bruggenkate et al, 1998
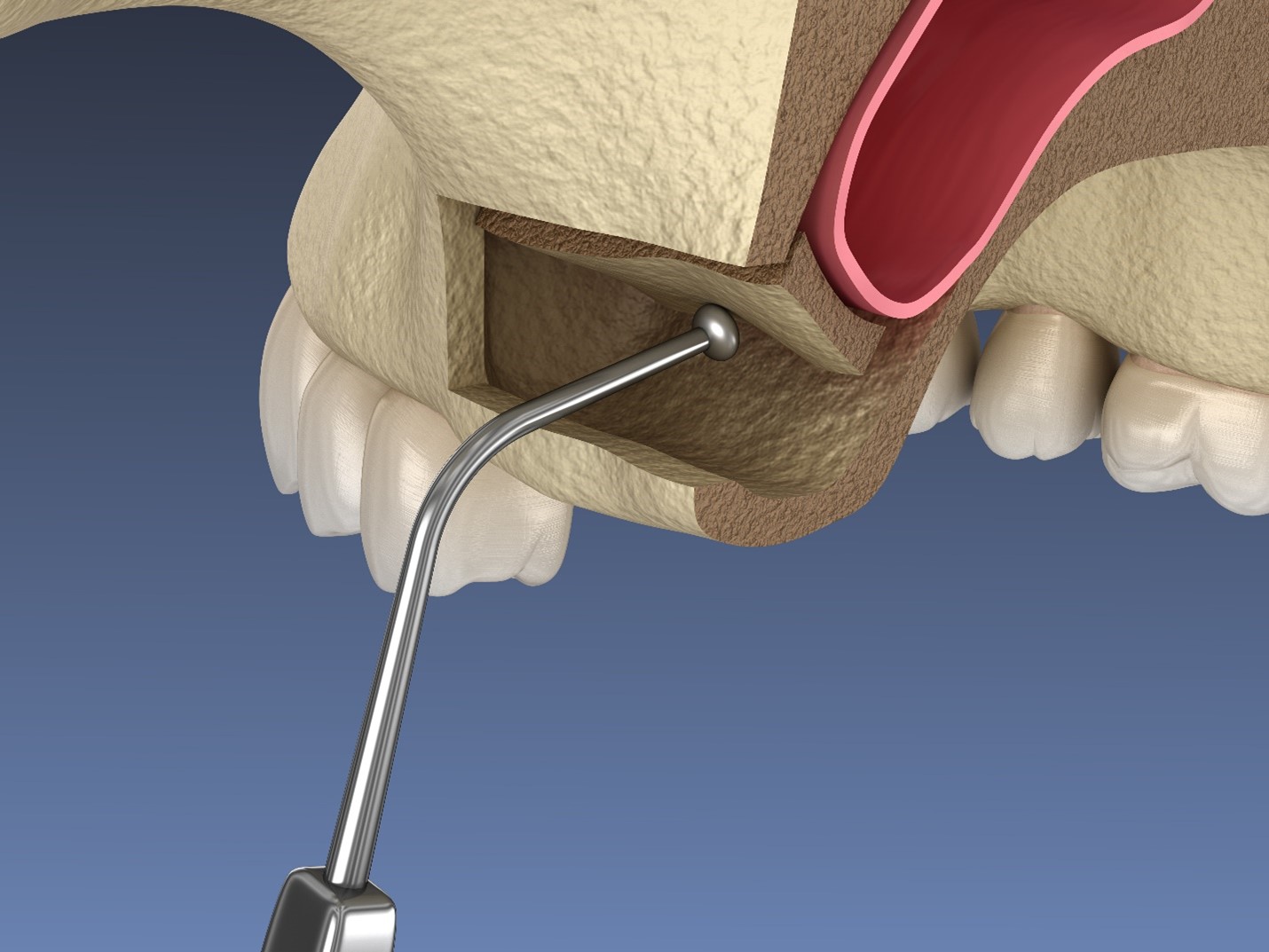
This paper describing Tatum’s “trap door” method of increasing the absolute bone height in the lateral maxilla.
Technique involves surgically creating a top hinge door in the lateral sinus wall, turning the door inward and upward together with the intact sinus mucosa, and filling the newly created space with bone graft.
Indications:
Insufficient bone height (< 10 mm) is available for dental implants or totally edentulous maxillae with insufficient bone height.
Contraindications:
A- Absolute:
Previous sinus surgery such as Caldwell Luc procedure
Maxillary sinus diseases such as tumors or chronic polypous sinusitis
Strong allergic conditions.
B- Relative:
Presence of Underwood’s septa or severe sinus floor convolutions
Contours of dental roots in the floor of the sinus
Extremely narrow sinus.
The gold standard graft material is autogenous(iliac crest, tibia head, chin, coronoid process, and/or lateral buccal cortical bone plate of the mandible) bone.
Implantations can be performed at sinus lifting (one-stage) or at a later date (two-stage).
1- One stage procedure:
Must have good quality and quantity of bone to provide good primary stability of the implant.
2- Two-stage:
When < 4 – 5 mm vertical bone height is available, ≥ 4 months after sinus lifting with autogenous bone.
Complications:
Perforation of the Schneiderian membrane (most common)
Infection
Possible loss of the graft into the sinus, and subsequent sinusitis.