
- By - Malfaifi
- Posted on
- Posted in التركيبات, التركيبات الثابتة, التركيبات المتحركة, تشخيص, زراعة الاسنان
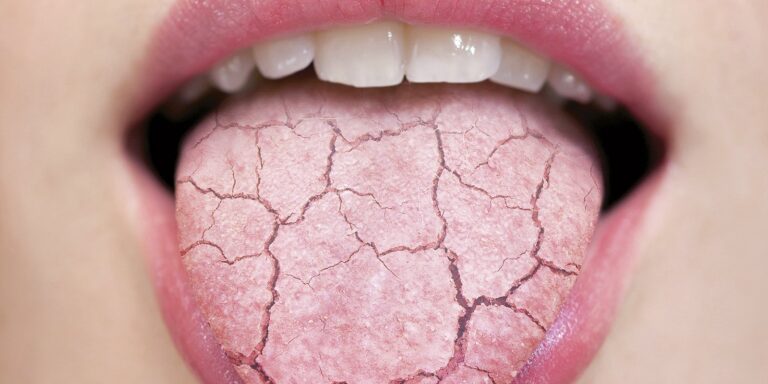
Xerostomia
Hyposalivation and Xerostomia: Etiology, Complications, and Medical Management
Turner 2016
· Hyposalivation: an objective finding of a decreased salivary production
· Xerostomia: the subjective feeling of having dry mouth
· Normal unstimulated flow rate: 800-1500 mL/day or 0.3-0.4 mL/min
· Abnormal flow rate: <0.1 mL/min
Normal Salivary Function
· 2 components: mucinous and serous, combined form whole saliva
· 3 types of major salivary glands: parotid, submandibular and lingual (sublingual) glands
· Parotid secretes mostly serous, sublingual and minor secrete only mucinous, and submandibular secretes both
· Salivary glands are innervated along the parasympathetic cholinergic pathway
Salivary Mucins
· Sequester water in the oral mucosa, acting as a lubricant and protective layer for the oral hard & soft tissues
· Major viscoelastic mucins are the gel-forming MUC5B mucin and the nonpolymeric MUC7 mucin
Salivary Minerals
· Saliva is rich in sodium, potassium, calcium, hydrogen, bicarbonate, phosphate, zinc, magnesium, and others
· Along with the salivary proteins, create an osmotic gradient between the intracellular fluid in the salivary cells and the extracellular fluid in the glandular ductules, which is the driving force that brings the intracellular fluid through the transmembranous channels into the glandular ductules.
· Normal oral pH: 6.0-7.0, stabilized by bicarbonate and phosphate ions
· Stable pH is necessary to activate salivary amylase (hydrolyses starch into sugars) and prevent overgrowth of Candida and other organisms
· Zinc is crucial for activation of taste buds (reason why hyposalivation patients have decreased/loss of taste)
Immune System Function
· Parotid glands contain B cells and plasma cells that excrete salivary Immunoglobulin A (IgA), which binds to bacteria, fungi and viruses, blocking microbial attachment
· Histatins, lactoperoxidase, lactoferrin, and secretory leukocyte protease inhibitor also play a role in immunity
Disease Entities
· Meta-analysis shows a prevalence that ranges from 5% to 47%
· 20% of the patients 65 years or older have some type of salivary gland abnormality
· Medication-induced hyposalivation is the most common cause in older adults because they take at least one xerogenic medication
· Other causes: Sjogren syndrome (SS) and head and neck radiation. Prevalence of hyposalivation is nearly 100%
Medicatioin-induced Salivary Gland Dysfunction
· >400 medications, and 80% of the most commonly prescribed meds can cause hyposalivation
· Incidence and severity of the hyposalivation are directly proportional to the number of medications that the patient is taking
· Medications that have an anticholinergic effect cause the most hyposalivation as they decrease the amount of Ach released by the parasympathetic nerves, disabling cell function.
· Most common xerogenic drugs: sedatives, antihistamines, anti-Parkinson, antihypertensive, & antidepressants
Radiation-Induced Hyposalivation
· When salivary glands are irradiated (60 Gy or more), it damages the salivary acinar and stem cells populations, causing permanent degeneration (atrophic, non-functional, fibrotic)
Sjogren Sydrome
· Autoimmune disease that targets salivary gland tissues. Salivary gland cells are infiltrated by plasma cells, B cells, T cells, macrophages, and mast cells
· Prevalence of SS varies 0.05% to 4.8%; Onset is typically between 40 and 50 yrs; female-to-male ratio of 9 to 1
Oral Effects of Salivary Gland Hypofunction
· Caries ( Strep mutans, protection by mucinous saliva, salivary debridement of teeth, & loss of buffering capacity), Candidiasis, Mucositis
· Management:
Xylitol, salivary substitutes, peripheral sialagogues and central sialagogues
· Salivary substitutes:
– Carboxymethyl cellulose, mucin, hydroxyethyl cellulose, water-glycerin, and glycerate polymer
– Viscosity is the most important physical property for the subjective relief of patients, followed by lubrication
· Peripheral Sialagogues: stimulate gustatory response; most common: ascorbic & malic acid; ineffective when there is a complete intrinsic damage to salivary gland cells; can demineralize tooth structure
· Mechanical Stimulation: can increase salivary flow from parotids by stretching the parotid capsule & compressing the parotid gland
Conclusions:
· Management of hyposalivation can be challenging
· No ideal agent is currently available to treat specific conditions effectively
· Practitioner must focus on prevention and treatment of complications of hyposalivation (caries, vulnerability to Candida infection, mucositis and sensation of xerostomia)